
By: Samantha Martin and Kristiina Rajamäki
Suomennos: Toistoa toiston perään: mikrosatelliittiepävakaiden kolorektaalisyöpien kaksi eri tyyppiä
Colorectal cancer is the third most common cause of cancer worldwide, including in Finland. The Finnish cancer registry reported 4,073 new cases and over 30,000 people living with colorectal cancer in Finland in 2022. There are also estimated to be over 10,000 individuals in Finland with Lynch Syndrome who are genetically predisposed, and so particularly susceptible, to developing colorectal cancer. The colorectal tumours of Lynch syndrome patients have a special characteristic: the tumour genome is full of mutations that slightly shorten or lengthen regions of repetitive DNA called ‘microsatellites’. This type of microsatellite unstable (MSI) colorectal tumour can also arise in the absence of genetic predisposition, referred to as a ‘sporadic’ MSI tumour. So does the tumour origin make a difference?
What is Lynch syndrome?

Lynch Syndrome is an inherited genetic syndrome which increases an individuals risk of developing several types of cancer during their lifetime, most commonly colorectal or endometrial cancer. In Lynch Syndrome, a mutated version of one of our mismatch repair genes is inherited. Mismatch repair is one of our many DNA repair systems and as the name suggests, is responsible for fixing mismatches that arise between the two DNA strands. Many of these mismatches naturally occur during DNA replication when a cell is dividing into two new cells; the mismatch repair machinery follows closely behind the DNA that is being copied to fix any mistakes that are made. We have two copies, or alleles, of each gene in each cell so the DNA repair mechanism is still able to function in a healthy Lynch Syndrome individual because of the remaining functional copy of the gene. However, if the second copy of the gene becomes mutated and stops functioning correctly, mismatch repair can be completely lost in a cell. Complete loss of mismatch repair leads to a large number of mutations accumulating and eventually, if the immune system is not able to eliminate the damaged cells, they will continue multiplying and develop into a cancer.
How are Lynch Syndrome tumours different to sporadic MSI tumours?
Tumours with a non-functioning mismatch repair system are known as microsatellite unstable (MSI) and make up about 15 % of colorectal cancers, while Lynch Syndrome only explains about 2-3% of colorectal cancers. This means that the majority of MSI tumours occur in individuals who do not have an inherited cancer syndrome, or in other words, are sporadic tumours. Individuals with a sporadic MSI tumour have not inherited a faulty allele of the gene and both alleles become mutated during their lifetime. In sporadic MSI tumours, the mismatch repair system is most often defective because of chemical tags preventing the mismatch repair gene known as MLH1 from being expressed, which means no MLH1 protein can be made. This is different to the mutations inherited by Lynch Syndrome individuals which are physical changes to the DNA sequence and mean the mismatch repair gene can still be expressed and create the protein, but the protein can’t function correctly.
Why do we want to compare them?
Lynch Syndrome and sporadic MSI tumours are often both caused by mutations in the same gene, MLH1, but have arisen by different pathways. Despite this, in research studies they are often grouped together as MSI tumours without taking into consideration whether the tumour has hereditary origins, so any differences between them might be missed. Even small differences between the tumours could potentially lead to big differences in how they respond to drug therapies. For example, immunotherapy drugs called immune checkpoint inhibitors that are increasingly often being used to treat MSI tumours, are much more effective in treating tumours in some individuals than others and we still don’t fully understand why. Additionally, the tools we have to study tumours are quickly improving and methods such as whole genome sequencing are becoming much more accessible and affordable. Therefore, the aim of our study was to compare sporadic MSI and Lynch Syndrome tumours using high-throughput sequencing technologies to improve our understanding of the ways in which they are similar and different.
What did whole genome sequencing tell us?
We collected MSI tumours from consenting patients across the south of Finland, along with healthy colon tissue nearby to the tumour, that is in any case removed during their surgery. From these tissue samples, we extracted both DNA and RNA and sequenced them. With the DNA we did whole genome sequencing to get the sequence of (almost) the entire genome. Everyone’s DNA is slightly different so we first compared the tumour DNA sequence to the DNA sequence of the same person’s normal colon tissue to identify what changes in the tumour are mutations.
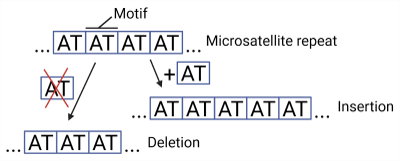
We looked at several ways the mutation landscape between sporadic and Lynch Syndrome might be different but overall we saw that these tumors are genetically very similar. Microsatellite repeats (repetitive regions of the genome where a short DNA sequence motif is repeated many times) accumulate a lot of small insertions or deletions in MSI tumours, and therefore they are more challenging to correctly sequence and are often disregarded when looking at mutations throughout the genome. We used a tool called ‘GangSTR’ to estimate how long each repeat is and to identify which repeats are mutated in the tumours, however found that the repeats were mutated similarly in both sporadic MSI and Lynch Syndrome tumours.
Another way we looked at the types of mutations in the tumours is by finding the mutation signatures. Mutation signatures are patterns of mutations across the whole genome which reflect the underlying process that caused the mutations. For example, a defective DNA repair system, UV radiation from sunlight, or tobacco smoking each leave their unique mutation signatures in the genomes of exposed cells. We looked at the signatures of single base mutations, and of insertions and deletions (collectively called indels). Once again, the mutation signatures were similar in sporadic MSI and Lynch Syndrome tumours.

We did, however, find that Lynch Syndrome tumours are made up of fewer cell subclones (cell populations carrying the same sets of mutations), which can be considered a sign of faster growth. This might be because Lynch Syndrome patients have developed a level of immunity against MSI tumours. Throughout their lifetime, their immune system has encountered and destroyed numerous similarly mutated cells that have a defective mismatch repair system, before any of these cell populations have managed to escape the immune cells and grow into a tumour. This could mean that mutated cells that have developed into tumours had to mutate and grow quickly to evade the immune response and survive.
What did RNA-sequencing tell us?
DNA is the blueprint sequence that stays in the cell nucleus and temporary copies of the DNA sequence are made by RNA. RNA molecules can then be used as a guide to make proteins or they can have roles in regulating which genes are expressed. We sequenced the RNA from the tumours which tells us how many copies of RNA matching each gene there were and, by extension, which genes are being most actively expressed in the tumour. When we compared sporadic MSI and Lynch Syndrome tumours we saw that there are 200 genes that are being expressed differently between the two tumour groups. To understand what these 200 genes might be doing in the tumours we looked at what functions these genes have and found that many of the genes had roles important to the immune system.
What comes next?
In summary, sporadic MSI and Lynch syndrome tumours are genetically very similar, but we noticed that there may be a difference in the role of the immune system in these tumours. In the next stage of this project we want to look into that more closely. This is important because the immune system is very active in MSI tumours and so immunotherapy is increasingly being used as a way to treat them. It is of importance to know if any underlying difference in the antitumour immune response could lead to differences in immunotherapy responses between sporadic MSI and Lynch syndrome tumours, and whether these tumour types should therefore be treated differently. Through collaboration and adopting different techniques, we will look more closely at the potential differences in the types of immune cells present in sporadic MSI and Lynch Syndrome tumours. Through this, we hope our work will benefit patients in the future by contributing to ongoing efforts to develop effective and targeted treatment options for these tumours.

Want to learn more about the Finnish Center of Excellence in Tumor Genetics?
Subscribe to the blog and keep up to date with the latest posts for a peek into the everyday life in cancer research. You can also follow us on Instagram (@tumorgenetics) and Twitter/X! (@CoEinTG)

One thought on “Every Repeat Counts: Two Different Flavours of Microsatellite Unstable Colorectal Cancer”
Comments are closed.