
By: Tomas Tanskanen, MD, PhD
Age is a strong risk factor for cancer. As the world’s population ages, the number of new cancer cases is increasing rapidly. What do epidemiological studies tell us about the relationship between age and cancer risk, and what challenges may lie ahead for aging populations?
Cancer in the Global Population
The world’s population has grown from 2.5 billion in 1950 to 7.8 billion in 2020. Over the same period, the number of people aged ≥65 and ≥85 years has increased from 130 million to 730 million and from 4.7 million to 64 million, respectively. Global life expectancy has increased dramatically from under 30 years in 1800 to 47 years in 1950–1955 and 72 years in 2015–2020. Early increases in life expectancy were largely attributable to reductions in child mortality, but in the later part of the 20th century, decreasing death rates at older ages have driven further gains in life expectancy.

The GLOBOCAN study by the International Agency for Research on Cancer estimated that 19 million new cancers occurred worldwide in 2020. Half of them occurred in people aged ≥65 years, although this age group represented only 9% of the world’s total population. The most common cancers diagnosed at ages ≥65 years were lung, colorectal, prostate, and breast cancer.
What We Have Learnt About Age and Cancer Risk
Early epidemiological studies on the relationship between age and cancer risk found that death rates for common cancers increased progressively with age. Based on a mathematical model, Armitage and Doll proposed the hypothesis that common cancers arise from normal cells through a process of perhaps 6 or 7 successive cellular changes. Genetic studies suggest that alterations in only 3 driver genes may be sufficient for the development of advanced solid cancers in adults, although every cancer is molecularly unique. The rate of multi-step cancer development depends on lifestyle habits, environmental exposures, and genetic factors such as smoking, sun exposure, and inherited or acquired defects in DNA repair genes.
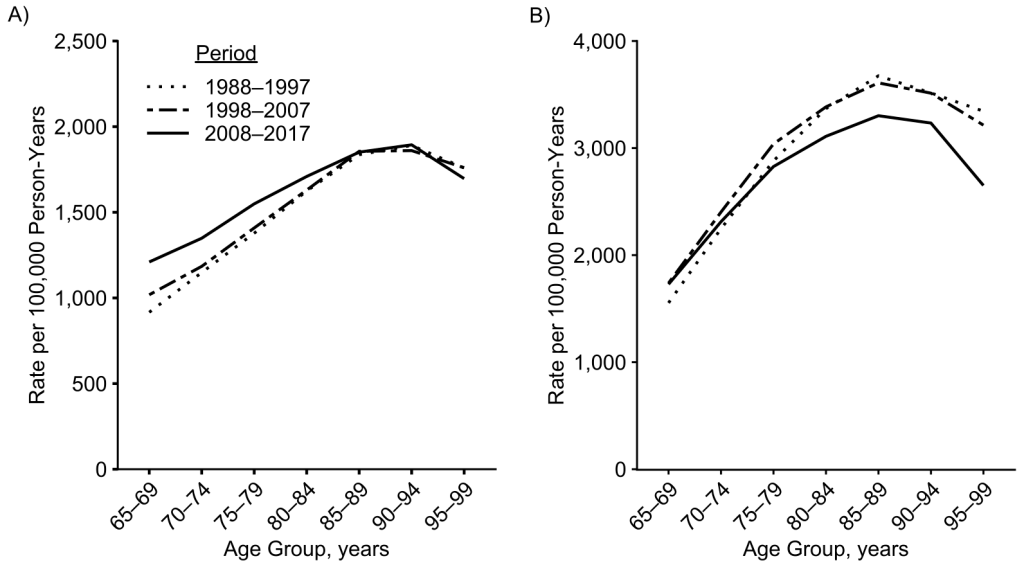
The Armitage-Doll model predicts that cancer rates increase with age across the entire human lifespan. In population-based epidemiological studies , however, cancer rates appear to peak at age 75–94 years and decline subsequently (Figure 1). The reason for the decline is unknown, but it might be due to undercounting of new cases at older ages, as well as age-specific differences in risk factors or biological characteristics.
Studying the Burden of Cancer in the Oldest Old
Population aging is expected to continue at a rapid rate in the coming decades, but relatively little is known about cancer in very old people. To study the burden of cancer in the oldest old, defined as age ≥85 years, we used data from the Finnish Cancer Registry, which maintains the national registry of all cancers diagnosed in Finland since 1953.
In Finland between 1953–1957 and 2013–2017, the proportion of new cancers diagnosed at ages ≥85 years increased from 1.5% to 9.6%, which corresponds to an increase from 600 to 15,000 new cases
Between the two latest study decades (1998–2007 and 2008–2017), the number of new cancer cases in the oldest old increased from 19,000 to 28,000. This increase was explained entirely by population aging and total population growth — there was no increase in overall cancer risk in the oldest old.

Photo by Noelle Otto from Pexels.com
What Are the Risks of Cancer in the Oldest Old
Cancer risk in the oldest old increased for certain cancer types such as lung cancer in women and skin melanoma in both sexes. Therefore, smoking and ultraviolet radiation, the major risk factors for lung cancer and melanoma, respectively, may be important avoidable causes of cancer even in the oldest old. Breast and uterine cancer, both of which have been linked to obesity, also showed increasing risks in the oldest old women.
Future Challenges
The growing burden of cancer in the oldest old has important implications for health care and future research.
Firstly, the diagnosis and treatment of cancer in very old people may be challenging because of coexisting chronic diseases, poor general health, and limited life expectancy. Therefore, we need a sufficient number of trained professionals in geriatric oncology and related specialties, and health care systems need to prepare for an increasing number of older patients with cancer.
Secondly, older patients have been underrepresented in clinical trials. More clinical trials are needed to evaluate the safety and efficacy of cancer treatments, especially anticancer drugs, in older frail patients.
Finally, epidemiological studies of cancer at extreme old age may generate new biological hypotheses for basic research.

