
By: Maiju Pankakoski
Suomennos: Elossa, mutta kuinka kauan?
Cancers are detected earlier than in the past. Early detection enables more successful treatment, but not always. In this text, I ponder how this phenomenon affects cancer statistics.
A cancer patient’s prognosis can be measured by using the relative survival ratio. It describes not only the severity of the cancer but also the diagnostics and the efficacy of treatments. Technically, the relative survival ratio is the proportion of cancer patients who are alive, for example, five years after the diagnosis, assuming that the cancer is the patient’s only possible cause of death.

However, the survival ratio does not tell how much of the patient’s life is lost due to cancer. The loss in life expectancy is another way to describe the patient’s prognosis. This method provides a concrete estimate of the years that the patient loses due to cancer, and it can be calculated for the remaining lifespan. Young cancer patients potentially lose more life years than older ones. Hence, the loss in life expectancy is a suitable measure for the loss caused by cancer at the societal level.
Illusions of Improvement
In Western countries, the prognosis of cancer patients has improved dramatically in recent decades. For example, in Finland, the age-standardized relative survival ratio for women with breast cancer has risen from 39% to 86% since the 1960s. Sixty years ago, breast cancer patients lived on average 13 years less than the general population, whereas today the loss in life expectancy is less than three years (*). The positive change is largely due to improved cancer treatments, but advanced diagnostics, such as cancer screening, also play a role. (*) I acknowledge Karri Seppä for calculating the survival rates and lost life years. The numbers are based on Finnish Cancer Registry data from 1953-1969 and 2005-2019.

The goal of screening is to reduce deaths caused by the screened cancer by detecting cancer at an early stage. Earlier diagnosis enables less invasive treatments and a better prognosis for the patient. Some types of cancer, such as cervical cancer, can be detected in the precancerous stage, and thus prevent the development of the cancer altogether. Some cancer types, such as breast cancer, are detected by screening as early-stage cancers. Breast cancer screening specifically aims to reduce mortality, or at least delay the time of death (without compromising quality of life).
Pitfalls of Early Diagnosis
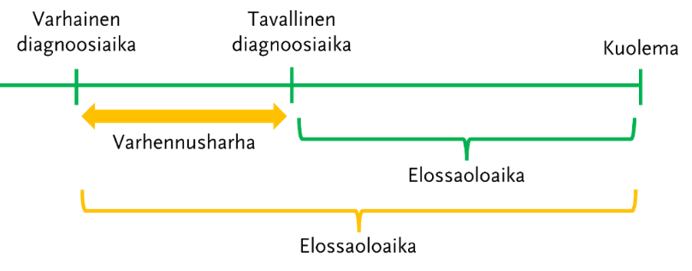
Sometimes, despite early detection of cancer, the patient’s life is not prolonged. The time of death is the same regardless of the timing of the diagnosis, and thus, screening does not lead to a better treatment outcome. This is reflected in the so-called lead-time bias (see image below), the overestimation of the survival ratio. Although the estimate seems to have improved, the patient has not gained additional life years. The quality of the patient’s life towards the end deteriorates when possibly heavy treatments are started unnecessarily early. This is in contrast to the idea of cancer screening which aims to improve the health of the population, not cause extra concern or useless treatments.
The impact of lead-time bias on a breast cancer patient’s survival was assessed in a Swedish simulation study, where the magnitude of the bias was calculated for different screening scenarios. The bias was greatest when assuming complete screening participation and high test sensitivity. Some differences in survival rates between population groups may be due to lead-time bias. Differences between socio-economic classes have previously been observed not only in breast cancer survival but also in screening participation. Comparing different time periods can also be sensitive to lead-time bias. The survival estimates presented at the beginning of this text are from decades ago when there was no screening yet.
The Value of an Effective Screening Program
Instead of relying on survival ratios, the effectiveness of screening should be evaluated using other metrics, such as the impact of screening on cancer mortality in the population. Although the harms associated with breast cancer screening are widely recognized, studies support population-based screening, and the EU also recommends it. An early-diagnosed localized cancer is usually much more treatable than a later-diagnosed metastatic cancer. Additionally, early detection can reduce the harms and costs of cancer treatments. However, the implementation of population-based screening programs must always be based on evidence of effectiveness, and the benefits must outweigh the harms. Screening programs must also be continuously evaluated and improved. The goal is to truly live as long as one would without having cancer.

Want to learn more about the Finnish Center of Excellence in Tumor Genetics?
Keep up to date with the latest tweets, videos and blog posts for a peek into the everyday
life in cancer research; subscribe to our blog and YouTube channel!
and don’t forget to follow us on Twitter (@CoEinTG)

One thought on “Alive- but for how long?”
Comments are closed.